Contact tracing & analytics: insights from a data-driven fight against Ebola and Malaria




The COVID-19 crisis and cascade of decisions to close workplaces, schools, restaurants and most other non-essential public spaces has been an unprecedented effort to protect family, friends and neighbours throughout our communities from the virus. Most of us have got the message to stay home, sing Happy Birthday twice while washing our hands and wear a mask when out on a walk. But for many, this is the first introduction to the fields of public health and epidemiology: you may have even heard the term “contact tracing” for the first time just this past week.
For epidemiology, this has been one giant teachable moment. Scientists and public health officials are suddenly all over the television and radio discussing the importance of tracking every possible interaction that could lead to the transmission of a disease to limit its spread.
If you’re already familiar with contact tracing, you may have Dr. Larry Brilliant’s 2006 TED Talk on the eradication of smallpox to thank. Brilliant described in great detail how he and a dedicated team traversed India to track down every case of smallpox, and every possible connection to each case, until they finally reached zero. He also predicted the challenge that we are facing now. Showing the simulation of an uncontrolled SARS outbreak that touched every country on Earth within three weeks, Brilliant ended with an unambiguous call to invest in systems for “early detection and early response” to limit the spread of disease.
At Tableau Foundation, we’ve seen just how effective contact tracing and thorough data collection can be for tracking and mitigating some of the world’s most destructive diseases. For years, we’ve partnered with non-profit organisations and local governments around the world to enable data-driven action in the fight against some of the world's deadliest illnesses: Malaria. Tuberculosis. HIV/AIDS. Ebola.
In every case, a key to controlling and eventually eliminating the spread of these diseases comes down to two very simple ideas: trace every possible contact with infected individuals, and keep information moving faster than the disease.
Learn more about Tableau Foundation’s work on the issue of global health.
Lessons from West Africa
Nowhere was this more evident than in the effort to fight Ebola in West Africa in 2014. Working through our partners at Dimagi and NetHope, and in partnership with The Earth Institute at Columbia University, we were able to deploy Tableau-powered analytics systems that enabled healthcare and policy leaders to see what steps they needed to take to reduce the potential spread of the disease.
While there was certainly a need for technology in collecting and analysing cases in Guinea, Liberia and Sierra Leone, the data collection methods were decidedly low-tech: conversations with infected patients about who they had come into contact with, how recently, and to the best of their ability, the names of others who those people might have been in contact with.
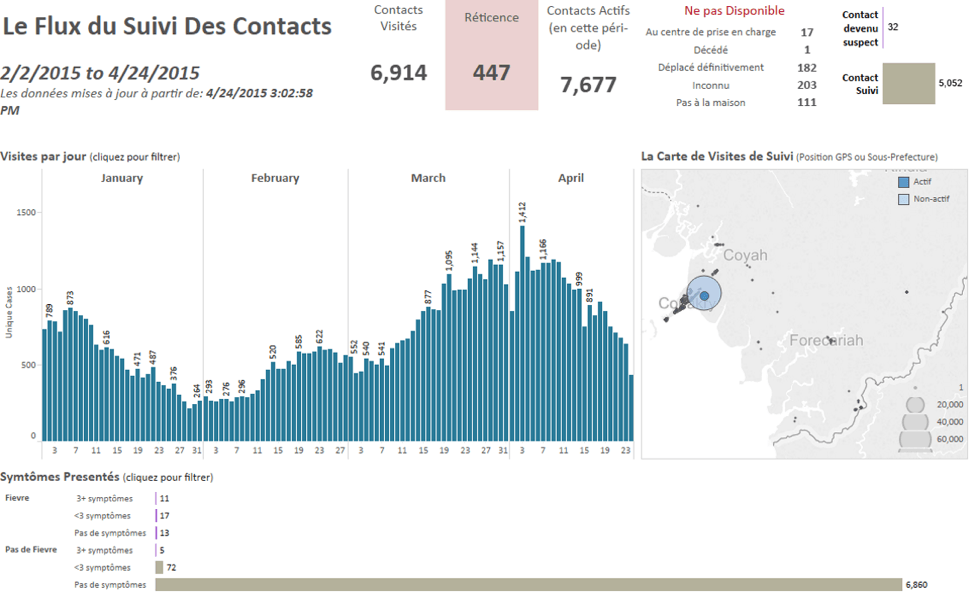
Summary dashboards from Guinea allow all agencies to understand the current state and progression of the outbreak.
These actions often required people to act in defiance of local custom and social norms, particularly in large families in close-knit communities where everything from communal eating to preparing the bodies of the deceased for funeral rites can allow a virus to pass from one human to another. People had to be educated about the nature of how the disease spread and encouraged to change those behaviours until the virus had been wiped out. And that knowledge would also become the foundation for the interviews conducted by health officials about any possible points of contact, as well as discussion of the steps taken to prevent transmission.
The addition of Dimagi’s technology to that workflow reduced the time it took for that data to be aggregated and visualised for local officials from a week to a couple of hours. Empowered with this data, they were able to methodically eliminate contact between infected individuals and the rest of the population. Eventually, this work halted the spread of a disease that infected over 19,000 and took the lives of over 7,500.

A leap forward in response planning
Much of this methodology was put to the test with a second Ebola outbreak in the Democratic Republic of Congo (DRC) in 2018. Our partner organization PATH was involved in a large public-private consortium that facilitated the rapid response to an outbreak in the Equateur Province. While health officials were equipped with an effective vaccine this time, contact tracing was critical to the process of officials determining where to deploy from their limited supply.
In the DRC, this contact tracing data was analysed at the national and regional Emergency Operation Centres (EOCs), alongside a variety of demographic, epidemiological and socio-economic data to determine where communities were most vulnerable and how to deploy resources in response. Both in person and virtually, leaders accessed these data for daily decision-making and understanding of the progress being made.
Informed by the lessons of the 2014 outbreak, the speed and effectiveness of the response in DRC unquestionably saved lives. At the end of 2019 – months after the initial cases were discovered – there were around 3,400 confirmed cases and 2,200 reported deaths attributable to the disease.
The Minister of Health in DR Congo reviews the Ebola dashboard from his tablet, keeping him connected in real time to the situation on the ground. Photo: Ministère de la Santé RDC, shared courtesy of PATH.org.
Finding the signal in the noise
While the symptoms and spread of the novel coronavirus is different than Ebola, it operates like any disease does. The virus is a passenger and the human body is the vehicle. What we know right now is that it spreads primarily through droplets generated when an infected person coughs or sneezes. Understanding and tracking these transmission methods – called disease vectors – is critical for limiting the spread of the disease. Contact tracing is simply the act of identifying people with active cases and then cataloguing every person they’ve come into contact with. Reuters recently published an article with terrific visualisations showing the process of tracking COVID-19 spread through selected South Korean communities.
The simple idea of contact tracing quickly becomes complex. While data is increasingly ubiquitous in much of our daily business and personal lives, data on these types of momentary or deeply personal interactions is much harder to come by.
"We’re working with a disease where time is of the essence. If you can’t control the contact tracing, you can’t control the disease."
The task of contact tracing is often made much more complicated – and more essential – by the incidence of asymptomatic carriers of the disease. Researchers are finding that COVID-19 may have significant rates asymptomatic carriers, which makes detection and tracing very difficult. If someone doesn’t even know they have the disease, they won’t immediately register in the data as a confirmed case – but if public health officials can trace their contact to a known case, they can be tested and assessed as a potential carrier.
COVID-19 is far from the only disease that often spreads via asymptomatic transmission. Around 80% of malaria carriers, for instance, don’t show the telltale signs of an infection: fever, shivers, nausea most visibly. Where a malaria treatment is available, surveilling, testing and treating can drive down infection rates. Where this is done well, we’ve seen an 80% reduction in reported malaria cases and a 90% reduction in deaths due to the disease. Contact tracing is essential to this success. When a case is diagnosed by a clinic, community health workers are sent back to that person's village to test everyone nearby for malaria, whether they show symptoms or not. Those that test positive are given medicine to treat it before it spreads to the entire community.
It is not hard to imagine how this translates to the experience we are all having with the coronavirus. Stay-at-home orders are designed to limit contact, but the virus can still network – perhaps undetected – through the limited family members, neighbours, service workers and others we may still be in contact with. As leaders start to develop plans for what “back to work” looks like, managing an inventory of those interactions is only going to get more complicated.
What comes next
As the conversation starts to turn to lifting some of the stay-at-home restrictions and restart parts of the economy, it is encouraging to see governors like Jay Inslee in Washington State prioritising contact tracing in their plans. That said, there are still more questions than answers about how this work will actually take place.
Apple and Google made headlines in the United States on 10 April when they announced a collaboration on a new platform for a voluntary contact tracing system through iOS and Android-powered devices. It was not the first effort to apply mobile technology – China, Singapore and South Korea are using similar strategies to trace interactions and notify nearby contacts of a potential carrier.
Dimagi, the same organisation whose technology was part of the 2014 Ebola response in Guinea, has partnered with 16 government agencies worldwide to deploy CommCare as part of the COVID-19 response strategy. One of those partnerships is with the Department of Public Health in San Francisco, which is working with UCSF to deploy CommCare as its primary contact tracing technology.
“When the time comes to make changes to the [stay-at-home] order, we need this contact tracing programme in place so that we’re equipped to respond to new cases and keep the virus from spreading out of control,” said San Francisco Mayor London N. Breed in a recent press release on the programme.
Through the CommCare platform, case contacts can choose to receive daily text messages or phone calls checking on their health and symptoms throughout the 14-day monitoring period. They can also choose to self-report symptoms via text, immediately alerting public health officials that follow up or testing may be required.
Tough work remains
However, we still don’t have clear answers to critical questions about data privacy and participation. Who would have access to the data and how would it be stored? Would users opt in to a limited, time-bound programme, or would it be an automatic enrolment process, where individuals would have to opt out of participating?
Add to that the equally important question about who would be left out entirely? The coronavirus response has laid bare for many the inequities of America’s digital divide. Lower-income communities – particularly communities of colour – are already experiencing a disproportionate number of lives lost. Would over-reliance on digitally-enabled contact tracing exacerbate those dynamics? Each and every one of these questions has had and deserves careful consideration; the debate about privacy and technology is one that has gone on for years and will likely continue for years to come.
Even with all the questions, we have learned through our work on Ebola and malaria that every day of inaction costs lives. We also have contact tracing as one of the most effective levers in public health and epidemiology that can be pressed right now to help limit the spread of the disease. Let's put that to work while making sure we ask ourselves the tough questions about equity and privacy, not just in our response to the pandemic but also in our recovery efforts. But let’s also not wait to settle those debates before acting.
This type of contact tracing may feel lo-fi to those of us in global tech hubs, but its long track record of success against some of the world’s most deadly diseases should outweigh the glow of innovation. These campaigns against Ebola and malaria were technology-enabled, but at the heart of the effort were people gathering information from patients and investigating their relationships.
That the technology may be more evolutionary than revolutionary should not deter us from embracing the moment. The contact tracing practices we can put in place today for understanding and limiting the spread of disease will reduce risk and save lives. We may be past the point of the “early detection and early response” Dr. Brilliant called for 14 years ago, but this is a moment where action can be the next step towards controlling – and eventually eliminating – the virus.
Related stories

After a year of COVID-19 charts, eight data communication lessons learned
 19 April, 2021
19 April, 2021

4 reasons why embedded analytics is your path to a new revenue stream in the COVID-19 era
This blog post covers four reasons why organizations should consider embedded analytics.

What we can learn from the public sector’s response to COVID-19
 21 May, 2020
21 May, 2020
A broad consensus is that COVID-19 will drive digital transformation in the public sector. During the 2020 Government Summit, speakers from Veteran Health Administration, Southwest Texas Regional Advisory Council, and FEMA discuss new processes, new technologies and innovations, and most importantly, a new mindset on decision making in the midst of crisis.
Subscribe to our blog
Get the latest Tableau updates in your inbox.